Adults: The dosage and duration of therapy shall be established depending on type and severity of infection and the condition of the patient.
The recommended daily dosage is as follows: 500 mg IV every 8 hours in the treatment of pneumonia, UTI, gynaecological infections such as endometritis.
1 g IV every 8 hours in the treatment of hospital acquired pneumonias, peritonitis, presumed infections in febrile neutropenic patients, septicaemia.
In meningitis the recommended dosage is 2 g every 8 hours.
A dose of up to 2 g three times daily in adults and adolescents and a dose of up to 40 mg/kg three times daily in children may be particularly appropriate when treating some types of infections, such as nosocomial infections due to
Pseudomonas aeruginosa.
Regular sensitivity testing is recommended when treating
Pseudomonas aeruginosa infection.
There are limited safety data available to support the administration of a 2 g dose in adults as an intravenous bolus injection.
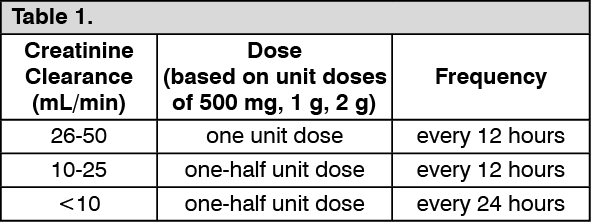
Dosage Schedule for Adults with Impaired Renal Function:
Dosage should be reduced in patients with creatinine clearance less than 51 mL/min, as scheduled as follows. There are limited data to support the application of these dose adjustments for a unit dose of 2 g. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Meropenem is cleared by haemodialysis and haemofiltration; if continued treatment with meropenem is necessary, it is recommended that the unit dose (based on the type and severity of infection) is administered at the completion of the haemodialysis procedure to restore therapeutically effective plasma concentrations.
There is no experience with the use of meropenem in patients under peritoneal dialysis.
Dosage in Adults with Hepatic Insufficiency:
No dosage adjustment is necessary in patients with hepatic insufficiency.
Elderly Patients: No dosage adjustment is required for the elderly with normal renal function or creatinine clearance values above 50 mL/min.
Children: For children over 3 months and up to 12 years of age the recommended dose is 10-20 mg/kg every 8 hours depending on type and severity of infection, susceptibility of the pathogen and the condition of the patient. In children over 50 kg weight, adult dosage should be used.
In meningitis the recommended dose is 40 mg/kg every 8 hours.
Febrile episodes in neutropenic patients-the dose should be 20 mg/kg every 8 hours.
There is no experience in children with renal impairment.
There are limited safety data available to support the administration of a 40 mg/kg dose in children as an intravenous bolus injection.
Method of Administration: Meropenem can be given as an intravenous bolus injection over approximately 5 minutes or by intravenous infusion over approximately 15 to 30 minutes using the specific available presentations.
Meropenem to be used for bolus intravenous injection should be constituted with sterile Water for Injections (5 mL per 250 mg Meropenem). This provides an approximate concentration of 50 mg/mL. Constituted solutions are clear, and colourless or pale yellow.
Meropenem for intravenous infusion may be constituted with compatible infusion fluids (50 to 200 mL).
Compatible solutions for reconstitutions of the powders: Dextrose 5% with potassium chloride 0.15%; Dextrose 5% in Ringer's injection, lactated; Dextrose 5% with sodium bicarbonate 0.02%; Dextrose 2.5% in sodium chloride 0.45%; Dextrose 5% in sodium chloride 0.2%; Dextrose 5% in sodium chloride 0.9%; Dextrose 5% in water; Dextrose 10% in water; Mannitol 2.5%; Mannitol 10%; Normosol M with dextrose 5%; Ringer's injection; Ringer's injection, lactated; Sodium bicarbonate 5%; Sodium chloride 0.45%; Sodium chloride 0.9%; Sodium lactate 1/6 M.
Compatible solution for infusion purposes: Dextrose 2.5% in sodium chloride 0.45%; Dextrose 5% and potassium chloride 0.15%; Dextrose 5% in Ringer's injection, lactated; Dextrose 5% in sodium chloride 0.2%; Dextrose 5% in sodium chloride 0.9%; Dextrose 5% in water; Dextrose 5% in water with sodium bicarbonate 0.02%; Dextrose 10% in water; Mannitol 2.5%; Normosol M with dextrose 5%; Ringer's injection; Ringer's injection, lactated; Sodium bicarbonate 5%; Sodium chloride 0.9%; Sodium lactate 1/6 M.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image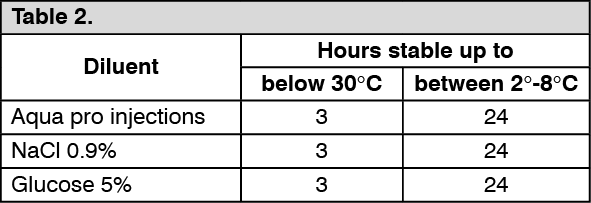 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
